
This post, predating my WordPress and even long-suspended Medium, was initially a collection of links I gathered for my first map activism account on Tumblr. It has been changed and updated over and over again, and will be updated more.
This version of the post is outdated and will be eventually replaced with this.
These are the misconceptions:
- Pedophilia is an “abuse fetish”/a treatable mental illness.
- “MAP” is a politically correct term made up to normalize pedophilia.
- DSM listed pedophilia as a sexuality by mistake.
- Pedophilia is illegal.
- All child molesters are pedophiles.
- All pedophiles offend.
- Therapy for MAPs involves building disgust towards the attraction.
- Communication with children increases risk of offense.
- Minors can’t be pedophiles.
- Pedophilia = pedophilic disorder.
- Pedophilia = POCD.
- MAPs can’t be LGBT.
- Maps aren’t oppressed.
- Stigma for MAPs is beneficial.
- MAPs don’t want to seek help.
OK, let’s start.
- Pedophilia is a fetish/a treatable mental illness.
The most common definition of a “fetish” is an “unusually strong liking or need for a particular object or activity, as a way of getting sexual pleasure.” (Collins Dictionary: https://www.collinsdictionary.com/dictionary/english/fetish). Basically, it means how or with what you want to have sex, not with who. Children aren’t an object or activity, what attracts pedophiles in children is their physical appearance and mentality. Moreover, pedophilia, unlike sexual abuse, may be linked to nurturing instincts and care rather than power. Psychologists agree that pedophilia cannot be treated.
“This opens the possibly that pedophilia is linked (in addition to or instead of an aberrant sexual system) to an over-active nurturing system”
Source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5778266/
“The majority (72%) of participants reported they had fallen in love with a child in their lifetime. Participants reported greater feelings of attachment to children than feelings of infatuation. Though sexual attraction and falling in love were strongly correlated, they were not synonymous.”
Source: https://sci-hub.se/10.1007/s10508-019-01579-9
“There is no evidence to suggest that pedophilia can be changed. Instead, interventions are designed to increase voluntary control over sexual arousal, reduce sex drive, or teach self-management skills to individuals who are motivated to avoid acting upon their sexual interests.”
Source: https://www.annualreviews.org/doi/10.1146/annurev.clinpsy.032408.153618
“Behavioral treatments such as aversion therapy and masturbatory reconditioning have shown some effect on arousal patterns, but do little or nothing to change underlying sexual desires (Laws & Marshall, 2003; Marshall & Laws, 2003; Seto, 2009). For the most part, cognitive-behavioral therapies designed to change the way pedophiles think, and act, have had little effect on either (Seto, 2009).”
Source: https://www.ipce.info/library_3/pdf/brian_cash_thesis.pdf
“There are no compelling data to suggest that pedophiles might be converted into teleiophiles(persons with a primary sexual interest in adults). Multiple types of interventions have been attempted, including sex-drive-reducing medications and talk therapies informed by any of many theoretical orientations. Although there exist authors who have claimed that their interventions changed their clients’ fundamental sexual interests (e.g., Fedoroff, 1988, 1992), such reports do not include comparison groups, long-term follow-up, or any validated, objective measure to verify the claims of successful change.”
Moreover, supposed pathologies in MAP brains were found out to be a result of an incorrectly conducted research, because in previous studies non-offending maps were not included.
“Our results are the first to demonstrate that executive dysfunctions are related to offense status rather than pedophilic preference.”
Source: https://pubmed.ncbi.nlm.nih.gov/28511726/
“Consistent with the conceptualization of the DSM-5, which specifies CSO as most the prominent criterion that differentiates pedophilia from pedophilic disorder, there were no significant differences between the GM volumes of the non-offending pedophiles and the teleiophilic controls. In contrast, the pedophiles who had engaged in CSO showed a significantly reduced relative GM volume in the right TP compared with pedophiles who did not. This difference was not attributable to age, level of education, IQ, sexual orientation, drug misuse/dependence, other Axis I or II disorders or general criminality.”
Source: https://www.nature.com/articles/tp201796
- “MAP” is a politically correct term made up to normalize pedophilia.
The term “MAP” was put in active use by B4U-ACT, a “a collaborative effort of mental health professionals and people who are attracted to children”, a world recognized organization aimed at help for MAPs and CSA prevention.
“ We use this term to refer to adults who experience feelings of preferential sexual attraction to children or adolescents under the age of consent, as well as adolescents who have such feelings for younger children. It is important to realize that these sexual feelings are usually accompanied by feelings of emotional attraction, similar to the romantic feelings most adults have for other adults. It is also vitally important to note that the presence of such feelings do not imply anything about behavior; non-criminological researchers note that many minor-attracted people live within the law (see our fact sheet). Such people are involved in the work of B4U-ACT, and more are known by people who work with B4U-ACT”
Source: https://www.b4uact.org/know-the-facts/faq/
“We started using the term MAP around 2007. The late Michael Melsheimer, our co-founder, introduced “minor-attracted person” as an alternative to “minor-attracted adult,” to reflect that most MAPs realize these attractions before they are adults themselves.”
Source: https://twitter.com/B4U_ACT/status/1178872015375290369
“A proposed alternative identifier is ‘‘minor-attracted people’’.
It gained popularity, because not every type of attraction towards a child/teen is pedophilia.
«I briefly review research on nepiophilia (infant/toddlers), pedophilia (prepubescent children), hebephilia (pubescent children), ephebophilia (postpubescent, sexually maturing adolescents), teleiophilia (young sexually mature adults, typically 20s and 30s), mesophilia (middle-aged adults, typically 40s and 50s), and gerontophilia (elderly adults, typically 60s and older) in the context of a multidimensional sexual orientations framework.»
Source: https://pubmed.ncbi.nlm.nih.gov/27549306/
- DSM listed pedophilia as a sexuality by mistake.
It is true that there was some scandal surrounded pedophilia. But not in the way you think.
“In the face of significant criticism of its inclusion in the DSM-5, the American Psychiatric Association (APA) has stated its intention to remove the term Pedophilic Sexual Orientation from the diagnostic manual.2 Removing that term in response to public criticism would be a mistake. Experiencing ongoing sexual attractions to prepubescent children is, in essence, a form of sexual orientation, and acknowledging that reality can help to distinguish the mental makeup that is inherent to Pedophilia, from acts of child sexual abuse.”
Source: http://jaapl.org/content/42/4/404.full
Researches addressed the fact that there are similarities between pedophilia and gender based attractions.
“By the above definition of sexual orientation — and most common definitions of sexual orientation — pedophilia can be viewed as a sexual age orientation based on the more limited evidence available regarding its age of onset, associations with sexual and romantic behavior, and stability over time. Though there are clearly differences in some respects, there are also striking similarities in the research literature on pedophilia.”
Source: https://www.scribd.com/doc/134033172/Michael-C-Seto-2012-ASB-is-Pedophilia-an-Orientation
“Sexual interest in children resembles sexual gender orientation in terms of early onset and stability across the life span. Although a genetic component to sexual interest in children seems possible, no research has addressed this question to date. Prior research showing familial transmission of pedophilia remains inconclusive about shared environmental or genetic factors. Studies from the domains of sexual orientation and sexually problematic behavior among children pointed toward genetic components.”
Source: https://www.jsm.jsexmed.org/article/S1743-6095%2815%2930336-2/abstract
- Pedophilia is illegal.
No. In all countries where such laws even exist, it’s sexual acts with children that are criminalized. For example, this is how it is formulated in US laws:
“Whoever, in the special maritime and territorial jurisdiction of the United States or in a Federal prison, or in any prison, institution, or facility in which persons are held in custody by direction of or pursuant to a contract or agreement with the head of any Federal department or agency, knowingly engages in a sexual act with another person who — (1) has attained the age of 12 years but has not attained the age of 16 years; and (2) is at least four years younger than the person so engaging; or attempts to do so, shall be fined under this title, imprisoned not more than 15 years, or both.”
Source: https://www.law.cornell.edu/uscode/text/18/2243
- All child molesters are pedophiles.
According to experts who work in the field of CSA prevention and study sex offenders, pedophiles are a minority among offenders.
- The Dunkelfeld project: 40% of molesters are maps. (https://www.praeventionstag.de/dokumentation/download.cms?id=2090 )
- an early Dr. Seto’s study: also 40% (https://www.researchgate.net/publication/24239585_Pedophilia )
- a Dutch study from 2015, the fullest piece of research on CSA I know: 20% (actually, it says 20% have any paraphilia at all, but I take it as the highest possible estimate of maps (https://www.dutchrapporteur.nl/Publications/OnsolidgroundTacklingsexualviolenceagainstchildrenintheNetherlands/index.aspx)
- an EPA entry: 16.2% (https://www.sciencedirect.com/science/article/abs/pii/S0924933814777314)
“Is sexual abuse motivated by sexual attraction? For the most part no, and in very rare cases, yes. However, these cases are not the norm, and motivations for child sexual abuse are numerous and complex, often particular to the abuser in question. Even abusers who have an attraction to children (pedophilia) may not be motivated by that attraction to abuse the child, it may be the result of the stigma or depression they feel from having the attraction and the flawed beliefs they may have about what a child is capable of handling.”
Source: https://www.csaprimaryprevention.org/CSA-FAQ.html
- All pedophiles offend.
Two official pieces of data are available to me.
“Bailey, Michael J., Paula A. Bernhard, and Kevin J. Hsu. “An Internet Study of Men Sexually Attracted to Children: Sexual Attraction Patterns.” Journal of Abnormal Psychology 125, no. 7 (2016): 976–88. https://doi.org/10.1037/abn0000212.
Out of their total responses, 371 people were excluded for not meeting the criteria of the study. Still, a total of 1,189 men did meet those criteria. Of those 1,189 men, 145 (12.2%) reported having a sexual offense conviction against a child. <…>
It is worth noting that their study pulled largely from support sites, and it could be theorized that people with prior child sex crime convictions may be more likely to seek out support than people with no such convictions.”
Source: https://www.csaprimaryprevention.org/prevalence-and-minor-attraction.html
4% maps committed a contact offense, and 9% – a child pornography offense.
I have conducted my own calculation, using the available statistics. With extremely unlikely and unfavorable of maps numbers, I got 40% maps being offenders. When I took more up-to-date and realistic numbers, I got 8% maps being offenders.
“Non-offending pedophiles are a unique population of individuals who experience sexual interest in children, but despite common misperceptions, have neither had sexual contact with a child nor have accessed illegal child sexual exploitation material. An emerging body of research has examined the prevalence of pedophilic interests, characteristics of non-offending pedophiles, correlates of pedophilic interests, and stigma associated with pedophilia. Treatment programs are beginning to produce findings regarding the effectiveness of treatment in supporting non-offending pedophiles to remain offence-free. The current review spans these areas of research and discusses potential treatment options for working with non-offending pedophiles based on that research base.”
Source: https://www.researchgate.net/publication/299657027_Non-Offending_Pedophiles
“Neurobehavioral models of pedophilia and child sexual offending suggest a pattern of temporal and in particular prefrontal disturbances leading to inappropriate behavioral control and subsequently an increased propensity to sexually offend against children. However, clear empirical evidence for such mechanisms is still missing. Using a go/nogo paradigm in combination with functional magnetic resonance imaging (fMRI) we compared behavioral performance and neural response patterns among three groups of men matched for age and IQ: pedophiles with (N = 40) and without (N = 37) a history of hands-on sexual offences against children as well as healthy non-offending controls (N = 40). As compared to offending pedophiles, non-offending pedophiles exhibited superior inhibitory control as reflected by significantly lower rate of commission errors. Group-by-condition interaction analysis also revealed inhibition-related activation in the left posterior cingulate and the left superior frontal cortex that distinguished between offending and non-offending pedophiles, while no significant differences were found between pedophiles and healthy controls. Both areas showing distinct activation pattern among pedophiles play a critical role in linking neural networks that relate to effective cognitive functioning. Data therefore suggest that heightened inhibition-related recruitment of these areas as well as decreased amount of commission errors is related to better inhibitory control in pedophiles who successfully avoid committing hands-on sexual offences against children. Hum Brain Mapp 38:1092–1104, 2017.”
Source: https://pubmed.ncbi.nlm.nih.gov/27767244/
- Therapy for MAPs involves building disgust towards the attraction.
Many researches pointed out harm that comes from stigma surrounding pedophilia. That’s why modern therapy for MAPs is aimed at self acceptance.
“The (im)mutability of pedophilia is a key aspect of helping non-offending pedophiles manage their sexual arousal and to refrain from offending. The accrual of empirical data exploring this issue is central to understanding and providing treatment to non-offending pedophiles: If pedophilia is immutable, then treatments for these individuals need basically to focus on coping with and managing pedophilic interests while leading a meaningful and fulfilling life and not on changing the person’s basic orientation. Whereas some authors have claimed that pedophilic interests may remit [11, 12], reanalysis of these data and methodological and statistical issues identified by other authors suggest that no such changes in orientation actually occurred [13–16].
Professionals helped some of these men accept their pedophilic interests by separating their sexual attraction from their sexual behavior and by managing their sense of selves (e.g., distancing themselves from stories of “child rapists” [25•, p. 8]). Engaging with other pedophilic individuals helped these men see that others with their interests were able to avoid offending, which brought a sense of hope. Having other social supports that knew about their interests helped because their supports could help them maintain boundaries with children, challenge potentially distorted thinking, and provide them with feedback regarding their behavior with children.”
Source: https://www.ipce.info/library/journal-article/non-offending-pedophiles
“The preferred model of treatment is LGBT affirmative psychotherapy, which treats sexual feelings as innate, unchangeable and subject to personal acceptance. The American Psychological Association provides guidelines on its website (see below). Applied to the minor-attracted person, affirmative therapy separates sexual orientation from its expression, emphasizing acceptance and personal growth. This in no way endorses sexual contact between adults and minors.”
Source: https://www.b4uact.org/gallery-2-columns-filter/psychotherapy-for-the-map/
“The primary aims of these approaches can be summarized as follows:
- To accept MAPs’ sexual orientation as stable and unlikely to change;
- To help MAP patients learn to live with their sexual feelings in a healthy way, most importantly without engaging in behavior that is illegal and/or harmful to children;
- To help patients develop self-acceptance via a positive but realistic self-concept, without resorting to cognitions that rationalize and normalize adult–child sexual activity in a maladaptive strategy to protect self-esteem; and
- To help patients learn to cope adaptively with the intense societal stigma against MAPs.”
- Communication with children increases risk of offense.
Experts no longer think so.
“Among pedophilic men, social contact with children has been discussed as creating a risk situation for sexual abuse. Also, pedophilic men searching for such contact are seen as harboring more beliefs legitimizing sexual contact with children. However, social contact may also decrease false beliefs. We tested these competing views in an anonymous Internet survey with a non-forensic, non-clinical sample of 104 self-classified pedophilic men. Results showed that both increased social and physical contact were significantly linked to fewer legitimizing beliefs toward sex with children, even when controlling for past psychotherapy, educational level, social desirability, and age.”
Source: https://drive.google.com/file/d/1GLKvyvTKbU6LBIVwzV_Ej7R_q1BZJqzz/view
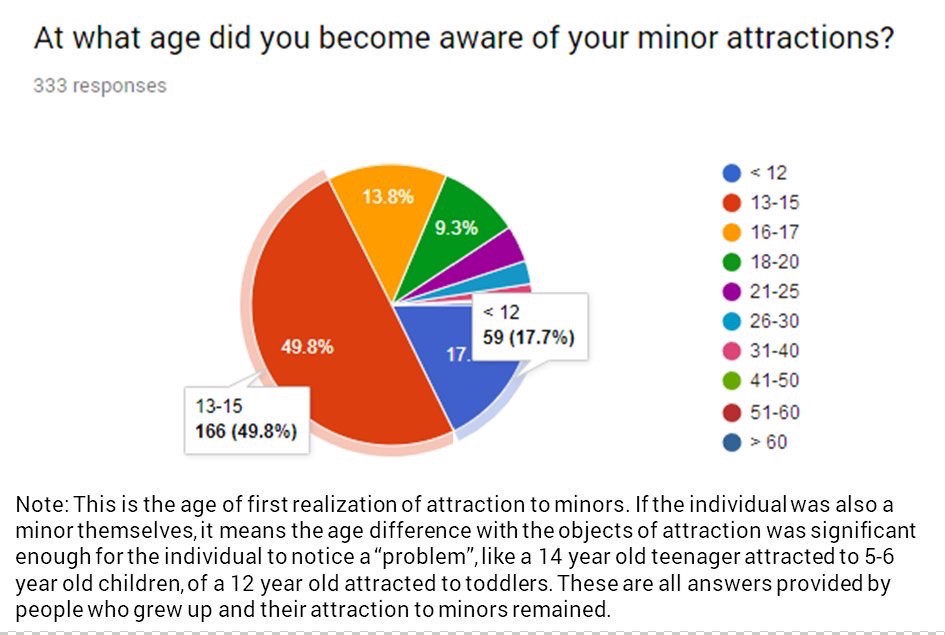
- Minors can’t be pedophiles.
“The study reveals that minor-attracted people become aware of their sexuality at an early age, experience stress caused by real or perceived societal rejection, and encounter both positive and negative reactions upon disclosing their identities. The conclusion underscores the need for a new approach to dealing with minor-attraction in contemporary Western society. I offer eight recommendations for instituting a strategy which incorporates empathy, education, and anti-discrimination measures.”
Source: http://summit.sfu.ca/item/13798
Most common age of first realization is 14
Source: https://www.b4uact.org/research/survey-results/youth-suicidality-and-seeking-care/
“Many participants struggled with acknowledging pedophilic interest in early puberty and experienced psychological difficulties as a result. Furthermore, many committed sex offenses during adolescence, while still discovering their feelings. Early recognition of risk factors and early start of interventions seems vital in preventing offending. Moreover, results suggest that risk for offending can be diminished by creating more openness about pedophilia and by providing pedophiles with social support and control.”
There is also this old poll, released by Ender.
Source: https://enderphile.wordpress.com/2018/09/11/growing-up-a-pedophile/
- Pedophilia = pedophilic disorder.
Many articles include references to the so called “pedophilic disorder”, and some people wrongfully believe that this is the correct medical name for pedophilia. In fact, there are different things.
“Pedophilia is defined as an ongoing sexual attraction toward pre-pubertal children (Freund, 1963, 1967; Seto, 2009). In the new DSM-5, pedophilia is de-pathologized by differentiating between the sexual preference for prepubescent children (i.e., pedophilia) and the disorder in case of additional factors. These factors include experiencing significant distress and impairment by fantasies and urges, or the acting out on behavioral level, including child pornography consumption and/or committing hands-on CSA offenses.”
Source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4478390/
“Pedophilic disorder can be diagnosed in people who are willing to disclose this paraphilia as well as in people who deny any sexual attraction to children, despite objective evidence of pedophilia. For the condition to be diagnosed, an individual must either act on their sexual urges or experience significant distress as a result of their urges or fantasies. Without these two criteria, a person may have a pedophilic sexual orientation but not pedophilic disorder.”
Source: https://www.psychologytoday.com/us/conditions/pedophilia
Pedophilic disorder is characterized by a sustained, focused, and intense pattern of sexual arousal — as manifested by persistent sexual thoughts, fantasies, urges, or behaviours — involving pre-pubertal children. In addition, in order for Pedophilic Disorder to be diagnosed, the individual must have acted on these thoughts, fantasies or urges or be markedly distressed by them. This diagnosis does not apply to sexual behaviours among pre- or post-pubertal children with peers who are close in age.
Source: https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/517058174
This aligns with what DSM says about other paraphilias.
“In contrast, DSM-5 redefines the term paraphilia so that it now refers to a persistent, intense, atypical sexual arousal pattern, independent of whether it causes any distress or impairment, which, by itself, would not be considered disordered. DSM-5 instead uses the term paraphilic disorder to refer to the disorder-worthy entities included in The Manual, which are defined as persistent and intense atypical sexual arousal patterns that are accompanied by clinically significant distress or impairment. Concomitant with this name change, DSM-5 also introduces the novel distinction between ascertaining a paraphilia and diagnosing a paraphilic disorder.”
Source: http://jaapl.org/content/42/2/191
- Pedophilia = POCD.
POCD is a type of OCD characterized by intrusive thoughts concerning harming children.
“Specifically, clients with pedophilia-themed OCD (P-OCD) experience excessive worries and distressing intrusive thoughts about being sexually attracted to, and sexually violating, children. Expressing these concerns may provoke misjudgments from uninformed mental health professionals that a client is presenting instead with pedophilic disorder. This misdiagnosis and subsequent improper interventions can then contribute to increased fear, anxiety, and in many cases, depression, in affected clients. Therefore, it is imperative that mental health professionals first possess a good understanding of this common manifestation of OCD. As such, in this article, we described obsessions and compulsions typical of P-OCD, in order to inform the reader of the distinctive differences between P-OCD and pedophilic disorder.”
Source: https://pubmed.ncbi.nlm.nih.gov/28822003/
- MAPs can’t be LGBT.
It is one thing to say that being a MAP doesn’t make you LGBT by default. But there are MAPs who are also queer, and they make up the majority of the map community.
According to an official survey, 75% of the map community are not heterosexual.
My two polls, run on Tumblr and Twitter, give the number of queer maps as 89.2% and 87.5% accordingly.
- Maps aren’t oppressed.
“As noted above, MAPs grapple with enormous social stigma, regardless of whether or not they pose any actual danger to children (Jahnke, Imhoff, & Hoyer, 2015; Jahnke, Philipp, & Hoyer, 2015; Jahnke, Schmidt, et al., 2015). In fact, it is reasonable to presume that MAPs encounter far greater stigma than do sexual minorities who are attracted to adults or age-peers.”
- Stigma for MAPs is beneficial.
“There is an emerging consensus among researchers that having pedophilic interests is not synonymous with child sexual abuse or other amoral behavior. Nevertheless, misconceptions about pedophilia are highly prevalent among the general public and mental health practitioners. <…> We argue that stigmatization of people with pedophilic sexual interests has undesired indirect effects on risk factors for child sexual abuse, particularly on an emotional and social level. Also, fear of being rejected or treated unethically may prevent pedophilic individuals at risk for sexual offending from confiding in medical practitioners or psychotherapists. Psychologists working with pedophilic individuals in forensic or clinical settings should be aware that stigmatizing people with pedophilia may increase their risk of sexual offending, and provide help to deal with potential stigma-related repercussions.”
“Stigmatization and societal punitiveness about pedophilia have a range of potential consequences, such as the social isolation of people with sexual interest in children, and the formation of policies that are not consistent with empirical research findings. Previous research has shown that people with pedophilic sexual interests use societal thinking to self-stigmatize, which in turn may actually serve to increase their risk of committing a sexual offense.”
“Results revealed that the shame and secrecy resulting from stigma associated with pedophilic interests often prevented our respondents from seeking professional counseling, and only about 20% tried to talk to anyone about their sexual interests prior to their arrest. Barriers to seeking and receiving psychological services included concerns about confidentiality, fears of social and legal consequences, personal shame or confusion about the problem, affordability, and challenges finding competent therapists who were adequately equipped to help them. Understanding and ultimately reducing obstacles to help-seeking can improve the quality of life for people with harmful sexual interests and potentially prevent sexual abuse of children or other vulnerable individuals.”
“In the general public however, it is to be expected that sexually abusive behavior towards children is often confused with pedophilia as a sexual preference. In the media, people with pedophile or other paraphile interests are often stereotypically portrayed as violent criminals (Diefenbach, 1997; Kitzinger, 2004). The public’s view of sexual offenders is extremely negative (Fortney, Levenson, Brannon, & Baker, 2007). Agreement with the stereotype that pedophilia often or always coincides with child sex offenses is likely to prompt a high degree of discrimination against people with pedophilia, regardless of their actual behavior. This may have a negative impact on the mental health of a person suffering from pedophilia, and unwanted indirect effects on the likelihood of this person seeking therapy when needed. Both potential consequences may, presumably, put children at risk of child sexual abuse.”
“For instance, the societal rhetoric about people who abuse children (e.g., “monsters,” “predators,” and “deviants,” along with declarations that they are not amenable to treatment and will inevitably reoffend) is rather damaging to the self-concepts of MAPs, who internalize these stigmatizing perceptions (Buckman et al., 2016; Jahnke, 2018). The shame and secrecy that result from this stigma prevent MAPs from reaching out to find role models, professionals, or confidants who might offer support or advice about how to deal with minor attraction and achieve a satisfying and healthy life (Beier, 2016; Buckman et al., 2016; Piché et al., 2016).”
Source: http://sci-hub.tw/10.1177/1079063218797713
- MAPs don’t want to seek help.
“A nonrandom, purposive sample of MAPs ( n = 293, 154 completed all questions) was recruited via an online survey. Results show that 75% of participants did seek formal help from a professional; however, just less than half of them found the experience to be helpful.”
Leave a Reply